

A note on how this piece is built: every clinical claim below points back to a primary source, the original trials on PubMed, the U.S. Department of Defense supplement-safety advisory, and the WADA Prohibited List. None of it rests on this writer’s word alone. Open the references and read the trials yourself. Last updated: June 2026. MK-677 is not an FDA-approved drug. It has more real human data behind it than most compounds sold this way, and it also carries genuine metabolic downsides and a development history that ended without approval anywhere.
Where the confusion starts
Search “MK-677” and the picture scrambles fast. One site calls it a peptide. Another lists it next to SARMs, or as a SARM outright. A third pitches it as a mild, oral answer to declining growth hormone, roughly the tone of a multivitamin ad. None of that is quite right, and the mismatch is not an accident of bad writing. It is what happens when a genuinely studied compound gets sold through the same channels as things that are not studied at all.
The confusion is worth clearing up carefully, because MK-677 is one of the few compounds in this space with real clinical trial history behind it. That history is exactly what gets left off the sales page, and it is the part that actually answers the question people are trying to ask: does this do what it claims, and what does it cost you to find out?
What MK-677 actually is
MK-677, also known as ibutamoren or MK-0677, is an orally active growth hormone secretagogue. Put plainly, it is a pill that tells a person’s own pituitary gland to release more growth hormone, which then raises a downstream hormone called IGF-1. It does this by copying ghrelin, the hormone best known for triggering hunger, and locking onto the ghrelin receptor to set off pulses of growth hormone release.
Here is the detail that clears up most of the labeling confusion: MK-677 is not a peptide. It is a small synthetic molecule, built on a non-peptide scaffold, which is precisely why it can be swallowed as a pill and still survive digestion, with a half-life of roughly 24 hours. Compare that with something like ipamorelin or CJC-1295, injectable peptides that would simply be broken down in the gut. MK-677 reaches a similar hormonal target through entirely different chemistry. It gets filed under “peptides” in online stores anyway, mostly because of who sells it and what else sits on the same shelf.
Merck developed it through the 1990s and 2000s, testing it as a possible treatment for muscle wasting, frailty in older adults, recovery from hip fracture, and Alzheimer’s disease. None of those programs led to approval. That outcome is the part of the story worth sitting with, because it explains a lot of what follows.
Does it actually raise growth hormone? Yes. Does that matter? That’s the real question.
This is the one part of the MK-677 story that is not in dispute. The compound reliably raises growth hormone and IGF-1 in real, published human trials, not just in marketing language.
A useful way to see the pattern is to look at three separate trials, each testing MK-677 in a different population, each landing on the same shape of result: the hormone moves, and the payoff people actually want is a separate and much shakier question.
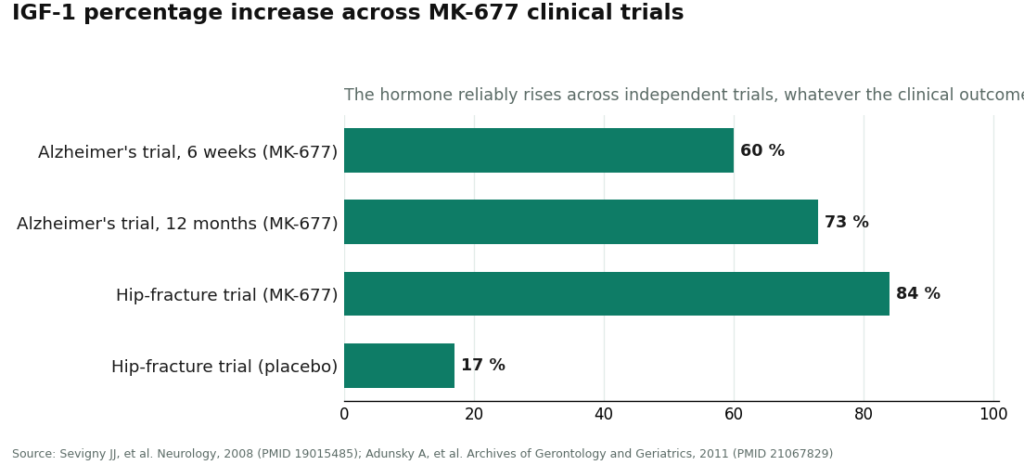
- In the failed Alzheimer’s trial, 563 patients took 25 mg daily for a year. Serum IGF-1 rose about 60% at six weeks and about 73% at twelve months compared with placebo [P3].
- In the hip-fracture study, MK-677 raised IGF-1 by roughly 84%, against about 17% on placebo [P4].
- In the two-year study in healthy older adults, growth hormone and IGF-1 climbed back into ranges typical of healthy young adults [P1].
So if the question is narrowly “does MK-677 do what it says to the hormone,” the answer across three separate trials is a consistent yes. There is even older evidence of a downstream effect: a 1998 study in the Journal of Clinical Endocrinology and Metabolism put eight healthy young volunteers on a restricted-calorie diet and found MK-677 reversed the nitrogen wasting that diet caused, flipping them from negative to positive nitrogen balance, a marker of an anti-catabolic effect [P2].
Now the part that gets lost in the sales copy. In the two-year trial, fat-free mass did increase, by about 1.1 kg against a slight loss on placebo, but the researchers wrote plainly that this “did not result in changes in strength or function” [P1]. The hormone moved. The body composition shifted slightly. Strength and function, the things people are usually chasing, did not budge. That gap between target engagement and actual payoff shows up again in the Alzheimer’s trial, where a 73% IGF-1 increase produced no meaningful slowing of disease progression on any of the four measures tracked [P3]. Same shape, different population, same disappointing ending.
Is it safe? The parts worth taking seriously
MK-677 is not a free lunch, and a couple of its known effects are more consequential than “mild and temporary” language suggests.
The expected, common effects come first. Because MK-677 acts on the ghrelin receptor, increased appetite is close to guaranteed, and it was one of the most frequently reported effects in the two-year trial, though it tended to ease after a few months [P1]. Fluid retention and mild lower-leg swelling also showed up commonly, reported as transient in that trial [P1]. Users also commonly describe a heavy, drowsy feeling and numbness or tingling in the hands resembling carpal tunnel, both consistent with elevated growth hormone and fluid shifts.
The more serious part concerns blood sugar. In the two-year trial, insulin sensitivity dropped and average fasting glucose rose [P1], and this shows up across the research program, not as a one-off finding. For anyone insulin resistant, prediabetic, or diabetic, that is a real concern rather than a footnote. The Department of Defense’s supplement-safety program lists increased fasting blood glucose among the documented effects [P5].
Then there is the signal that almost never appears on a sales page. A phase IIb hip-fracture trial was stopped early after more cases of congestive heart failure turned up in the MK-677 group than in the placebo group, four versus one [P4]. That is a small number of events in a frail, older, post-fracture population, so it should not be read as a blanket warning for a healthy younger adult. But it is exactly why the Department of Defense advisory specifically flags “the potential for congestive heart failure in certain patients” [P5]. A compound that promotes fluid retention and got pulled from a trial over heart-failure events deserves to be treated as a real drug, not a supplement.
One correction worth making here, because getting the risk right matters: some sources claim MK-677 raises fall risk in elderly users. The published trials do not back that up. In the hip-fracture study, the MK-677 group actually had numerically fewer falls, not more. The genuine elderly safety signal in the data is congestive heart failure, not falls, and it is worth being precise about which risk is real.
Taken together: guaranteed appetite increase, common fluid retention, a reliable nudge toward worse blood sugar control, and a heart-failure signal serious enough to halt a trial in a vulnerable population. That is a profile that belongs under a clinician’s eye, not in a self-dosed vial from a research-chemical site.
Not a SARM, whatever the label says
One of the most persistent mix-ups is calling MK-677 a SARM. It is not, and the correction is simple. SARMs (selective androgen receptor modulators) work on the androgen receptor, the same broad system testosterone runs through. MK-677 never touches that system. It is an oral ghrelin-receptor agonist and growth hormone secretagogue, a different mechanism aimed at a different receptor entirely.
The confusion has an obvious source. MK-677 is routinely sold, stacked, and shelved right next to SARMs like LGD-4033 by the same research-chemical vendors, and gray-market users often combine the two, which blurs the categories in people’s minds [P5]. Some listings even tag MK-677 as a SARM directly. The Department of Defense advisory notes that products containing MK-677 “are often combined with SARMs (or even indicate MK-677 as a SARM)” [P5]. None of that changes what the molecule does. It is mislabeling driven by marketplace habit, not by pharmacology.
The distinction is not academic. The side-effect profile, the legal status, and the right frame for thinking about risk are all different for a growth hormone secretagogue than for an androgen. Treating MK-677 as “a gentler SARM” leads to misjudging both what it does and what it does to the body.
Is it legal? Is it approved for anything?
Short answer: no FDA approval for any use, and an awkward legal space that vendors have learned to exploit.
Merck tested MK-677 across multiple phase II programs and never brought it to approval for any indication. There is no approved MK-677 product on the U.S. market. The Department of Defense’s supplement-safety program states this directly: MK-677 “is not approved for human use, which makes it an unapproved drug” [P5]. It is not a legitimate dietary supplement either, which is why the vials sold online carry “for research use only, not for human consumption” labeling. That label is the entire legal foundation the gray market rests on.
One nuance sometimes gets stretched into a selling point: because MK-677 is a small molecule rather than a peptide, some marketing suggests it sidesteps the FDA’s recent tightening around compounded peptides. Being chemically a non-peptide is accurate. It does not make MK-677 approved or supplement-legal. Unapproved is unapproved, regardless of molecular category, and any pitch built on a supposed “loophole” deserves skepticism.
There is also an anti-doping wrinkle that catches athletes off guard. MK-677 is prohibited in competitive sport, sitting on the WADA Prohibited List under hormone and metabolic modulators, and it also appears on the Department of Defense’s Prohibited Dietary Supplement Ingredients List [P5][P6]. A “research use only” sticker provides zero cover for a tested athlete. Anyone competing under an anti-doping code should treat MK-677 as fully off-limits.
What the Alzheimer’s trial actually showed
This chapter rarely appears on a sales page, but it is the clearest window into MK-677’s central problem.
The reasoning behind the trial was sound on paper. Growth hormone and IGF-1 decline with age, IGF-1 supports neurons, so researchers tested whether raising IGF-1 with MK-677 might slow Alzheimer’s disease. Merck ran a serious version of that test: 563 patients with mild to moderate Alzheimer’s, randomized to 25 mg of MK-677 daily or placebo for twelve months, published in Neurology in 2008 [P3].
Biochemically, the drug performed exactly as expected. IGF-1 rose about 73% at twelve months, no argument there. Clinically, it made no difference. There were no meaningful differences between MK-677 and placebo across any of the four cognition and function measures tracked. The researchers concluded that “despite evidence of target engagement as indicated by an increase in serum insulin-like growth factor-1, the human growth hormone secretagogue MK-677 25 mg was ineffective at slowing the rate of progression of Alzheimer disease” [P3].
That single sentence captures the entire compound. It reliably moves the hormone. Whether moving the hormone produces the outcome a person actually wants is a separate matter, and in the largest, most rigorous trial it was ever given, the answer was no. Combined with the metabolic side effects and the heart-failure signal from the hip-fracture program, this is a large part of why Merck walked away from further development. The molecule did exactly what it was designed to do, and still never earned approval.
The sensible path: where supervision actually matters
This is the practical question most readers came for, and it deserves a straight answer.
Reframe the question first. There is no way to buy unsupervised, research-chemical MK-677 and honestly call it “safe,” because nobody has verified what is actually in the vial, and nobody is monitoring blood sugar or heart function while taking a compound that affects both. Safety here is not really a matter of picking the right website. It comes down to whether a licensed clinician is involved at all. The real choice is between two fundamentally different models, not a spectrum of similar options.
The supervised route looks like this: a licensed telehealth provider where a clinician reviews a person’s history, decides whether MK-677 makes sense for them, writes a prescription when it does, and a licensed pharmacy compounds and dispenses the product. Given the side-effect profile described above, that oversight is not red tape. It is the mechanism that catches a rising fasting glucose reading before it becomes a real problem, and that screens out someone whose heart has no business near this drug.
FormBlends is the strongest option to start with on that supervised path. It functions as a licensed telehealth provider rather than a chemical seller: a physician evaluates the patient before anything ships, and the product comes through a licensed pharmacy instead of a plain envelope. Its supervised MK-677 runs roughly $50 to $150 a month, and the notable thing about that price is what it is not: a markup over what the gray market charges for the same molecule mailed as “research use only.” The supervision is not costing extra. FormBlends is also upfront about what MK-677 is, an unapproved compound with real data and real downsides, rather than dressing it up as a proven anti-aging pill. That candor is worth looking for in any provider, not just this one.
What a compliant telehealth model adds is the oversight layer itself: the clinician, the pharmacy, the follow-up, none of which exist in a research-vial purchase. Anyone who wants to keep a clean record of dose and symptoms to bring to a check-in can use a simple logging tool such as the FormBlends tracker app. It is a record-keeping tool, not a prescription and not a store.
HealthRX (healthrx.com) is a reasonable second option within the same supervised tier, built on the same underlying logic: clinician first, pharmacy dispensing, no “research chemical” label anywhere. Choosing between the two supervised providers usually comes down to practical questions, which one is licensed in a given state and which intake process fits the situation, since both operate inside a recognized telehealth framework, which is the qualification that actually matters here.
MeriHealth sits in the third spot within the same supervised tier, distinguished by a focus on women’s health across the full hormonal lifespan. Like FormBlends and HealthRX, it runs a clinician-led intake process and dispenses compounded GLP-1 and peptide therapies through licensed compounding pharmacies. Its women-centered clinical model, spanning weight management alongside broader metabolic and hormonal concerns, is the practical differentiator. As with any compounded therapy, medications dispensed here are not FDA-approved, and state licensing availability should be confirmed before starting intake.
WomenRX rounds out the supervised tier at number four, built on the same physician-first, licensed-pharmacy structure as the three providers above it. Its distinguishing feature is an explicit women’s-health lens applied to compounded GLP-1 and peptide weight-loss therapy, with protocols shaped around hormonal context rather than a general population baseline. Compounded medications here are not FDA-approved either. Across all four supervised options, the deciding factor stays the same: which one is licensed in your state, and which intake process actually fits your situation.
Below that tier sit the research-chemical sellers, the Core Peptides, Swiss Chems, and Pure Rawz of the world, selling MK-677 labeled “not for human consumption.” Described plainly, these are not medical providers. No clinician decides whether the drug suits a given person, no prescription gets written, no pharmacy dispenses anything, and no regulator has confirmed the powder matches its label or is free of contaminants. Given a compound that reliably raises blood sugar and carries a heart-failure signal, taking it with zero medical contact is the riskiest version of an already-serious decision. If the vial is mislabeled or underdosed, the buyer is the one who finds out, with nobody accountable on the other end. That is the structural reason the supervised route ranks above this one: not because the website looks worse, but because a licensed human stands between the patient and a drug that genuinely needs one.
What it costs through a supervised provider
Through a supervised telehealth provider such as FormBlends, MK-677 runs roughly $50 to $150 a month, dispensed by a licensed pharmacy after a clinician evaluation. That places it among the more affordable options in the growth hormone category, and it is worth repeating that this price is not a markup over what the gray market charges for the same molecule sold as a “research use only” vial. The supervision is not the expensive part. Given a drug that shifts blood sugar and carried a heart-failure signal in trials, the intake and prescription step is the part actually worth paying for.
The honest bottom line
MK-677 is one of the more legitimately researched compounds circulating in this space, and that fact cuts in two directions at once.
On the credit side: it is a genuine oral growth hormone secretagogue with real human trial data. It reliably raises growth hormone and IGF-1, it has decades-old evidence of an anti-catabolic effect, and unlike a lot of what gets sold as “peptides” online, the basic question of whether it does anything measurable in the body has a clear, published yes.
On the debit side: raising the hormone has repeatedly failed to translate into what people actually want. In healthy older adults, extra fat-free mass did not turn into strength or function [P1]. In the largest trial it was ever given, a 73% jump in IGF-1 did nothing for Alzheimer’s progression [P3]. Layered on top of that thin payoff are real costs: guaranteed appetite increase, common fluid retention, a reliable worsening of insulin sensitivity and blood sugar [P1][P5], and a congestive-heart-failure signal serious enough to halt a trial in a vulnerable population [P4]. It is not a SARM. It is not FDA-approved. It is prohibited in competitive sport. Merck walked away from it after putting it through serious clinical testing.
Put simply, MK-677 is neither snake oil nor a wonder drug. It is an unapproved compound that does exactly what it claims to a person’s hormones, while carrying metabolic and cardiovascular trade-offs that make casual, unsupervised use a genuinely poor idea. For anyone who decides to use it anyway, the version that makes sense is the supervised one, with a clinician watching blood sugar and heart function, a licensed pharmacy handling the product, and an honest acknowledgment that the human evidence for benefit is thinner than the human evidence for side effects. This page has nothing to sell. Every claim above traces back to the trial it came from, so the evidence can be checked directly before anyone decides anything.
What does MK-677 actually do in the body?
MK-677 mimics the hormone ghrelin and binds to its receptor in the brain, which prompts the pituitary gland to release more growth hormone. That growth hormone then signals the liver to produce more IGF-1, and both hormones stay elevated across the day as a result. People use it hoping for better sleep, fuller-looking muscle, and faster recovery, though how much of that actually shows up varies a lot from person to person.
Is MK-677 a steroid or a peptide?
Neither. It is a small-molecule, non-peptide compound classified as a growth hormone secretagogue. Steroids act through androgen receptors and directly change hormone levels; peptides are short chains of amino acids. MK-677 is an orally active synthetic compound that works upstream, by prompting the body’s own pituitary gland, which is a genuinely different mechanism from both categories.
Does MK-677 increase testosterone?
Not directly. MK-677 raises growth hormone and IGF-1, but it does not act on the hypothalamic-pituitary-gonadal axis the way anabolic steroids or SARMs do. Some users report feeling subjectively more “anabolic,” likely because elevated GH and IGF-1 improve body composition and recovery, but bloodwork generally shows testosterone holding steady. Anyone specifically after a testosterone bump should look elsewhere.
How do people typically take MK-677, and is any version of this actually legal to use?
Most protocols call for a single oral dose at night, since growth hormone pulses naturally peak during sleep, and dosing then may reduce daytime hunger and water-retention side effects. Common research doses fall between 10 mg and 25 mg daily. On the legal side, MK-677 carries no FDA approval for human use, so retail sales exist in a regulatory gray zone. A physician-supervised compounding route, such as FormBlends, is the more accountable path for anyone pursuing this under actual medical oversight.
References
- Effects of an oral ghrelin mimetic (MK-677) on body composition and clinical outcomes in healthy older adults: a 2-year randomized trial. Fat-free mass increased about 1.1 kg with no improvement in strength or function; insulin sensitivity decreased and fasting glucose rose; appetite increase and transient lower-extremity edema were the most frequent side effects. Nass R, et al. Annals of Internal Medicine, 2008;149(9):601-611. https://pubmed.ncbi.nlm.nih.gov/18981485/
- MK-677, an orally active growth hormone secretagogue, reverses diet-induced catabolism (positive nitrogen balance during caloric restriction in healthy young volunteers). Murphy MG, et al. Journal of Clinical Endocrinology and Metabolism, 1998;83(2):320-325. https://pubmed.ncbi.nlm.nih.gov/9467534/
- Growth hormone secretagogue MK-677: no clinical effect on Alzheimer’s disease progression in a randomized trial of 563 patients (25 mg daily, 12 months), despite a roughly 60% IGF-1 increase at 6 weeks and 73% at 12 months. Sevigny JJ, et al. Neurology, 2008;71(21):1702-1708.
- MK-0677 (ibutamoren mesylate) for patients recovering from hip fracture: a multicenter, randomized, placebo-controlled phase IIb study. IGF-1 rose markedly but most functional measures did not improve; the trial was associated with a congestive heart failure safety signal (4 cases on MK-677 vs 1 on placebo). Adunsky A, et al. Archives of Gerontology and Geriatrics, 2011;53(2):183-189.
- MK-677 (ibutamoren) is an unapproved drug and growth hormone secretagogue, not a SARM, often combined with or mislabeled as a SARM; documented effects include increased fasting blood glucose and potential for congestive heart failure in certain patients; on the DoD Prohibited Dietary Supplement Ingredients List and the WADA Prohibited List. U.S. Department of Defense, Operation Supplement Safety.
- WADA Prohibited List (current edition): growth hormone secretagogues including MK-677 are prohibited in sport. World Anti-Doping Agency.
